
Did you ever have a lot of ear infections as a child? I did. A lot. One year, I had 14. I was little at the time, so it was a lot of crying, a lot of trips to the doctor’s office, and a lot of medicine. Finally, my pediatrician recommended, “tubes” for my ears. Being little, I didn’t even know what caused an ear infection; let alone why they wanted to put tubes in my ears. So in this blog post, you will get to learn what an ear infection even is, and what tubes are and if they even prove to be effective.

The top picture is a diagram of the inside of an ear. The bottom diagram shows a swollen ear.
First things first: ear infections. We have all had them, and if you haven’t you are lucky. Ear infections are much more common in younger children. The middle ear/eardrum are where the ear infection occurs. The middle ear is located between the eardrum and the inner ear. There are three tiny bones (the malleus, incus, and stapes) located within the inner ear that transfer sound vibrations from the eardrum to the inner ear. Ear infections are often bacterial or viral infections and develop when fluid builds up behind the eardrum. Otitis media with effusion (OME) is the thick fluid that builds up behind the eardrum, also known as an ear infection. The eustachian tube (see diagram) connects the ear to the back of the throat. The eustachian tube’s job is to drain fluid from the ear, and is then swallowed. Ear infections occur when the eustachian tube is partially blocked, causing the fluid to build up and not properly drain. The eustachian tube can become blocked from drinking while lying down, and a sudden increase in air pressure. Swelling of the eustachian tube can happen from allergies, irritants, and respiratory infections. Long-term problems consist of persistent fluid in the middle ear or frequent infections (me!) can lead to hearing problems, spread of infection, or tearing of the eardrum. That’s why it is important to consider options to fixing the problem, with the most popular being ear/ventilation tubes!

This diagram illustrates a fluid filled middle ear and where the small incision is made in the ear drum to help drain the fluid
Ear tubes are usually inserted in children’s ears, but can be placed into adults. The scientific term for the surgery is called myringotomy (this is just the process of making an incision), but ventilation tubes are usually inserted in the incision to keep it open longer and prevent better drainage and longer relief. The surgery is done while the patient is under general anesthesia. The ear tube procedure consists of making a small surgical incision (myringotomy) in the eardrum of the infected ear(s). Any fluid is removed with suction through this cut before the tube is inserted. A small cylinder (tube) is placed through the eardrum. The tube is bigger on the edges so it stays in place in the eardrum. The tube is hollow and allows air to flow so pressure remains the same on both sides of the eardrum. When air is able to get behind the eardrum (through the tube), it allows trapped fluid to flow out or dry up. Overall, the surgery is an easy procedure, and an overnight stay is not required. Doctors may prescribe eardrops or antibiotics for after the surgery. After a few years, the tubes are supposed to be “pushed out” of the eardrum by themselves. If they do not fall out on there own, they can be surgically removed (this is what happened with mine). The hope is that ear infections will stop once one round of tubes are done, but if ear infections return, another set of tubes can be inserted. This is the most common surgery to help relieve reoccurring ear infections in young children.
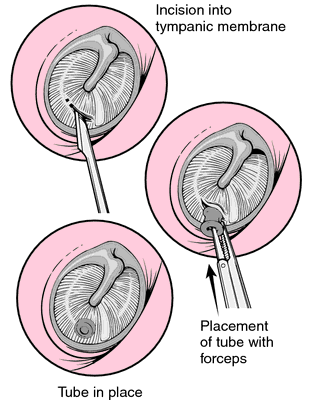
This diagram is another view of the small incision (myringotomy) being made in the eardrum. This diagram also shows the placement of a ventilation tube placed in the eardrum.
So is getting tubes effective? Is there a better option? While a myringotomy is the surgery, there was a study done to test the effectiveness of two procedures commonly done to people with multiple ear infections. While inserting ventilation tubes is the most common surgery, a laser myringotomy is becoming more popular. “Laser myringotomy has prove to be a safe method to ventilate the middle ear, and results of up to 70% efficacy have been reported. However, the indication for laser myringotomy is not yet known, and evidence is lacking that laser myringotomy is an alternative or ventilation tubes.” The study was conducted in seven Dutch hospitals from July 1999 to September 2001. Children included in the study were less than 11 years old, and parents had noticed impaired hearing during at least 3 consecutive months. Children who previously had laser myringotomy or ventilation tubes were excluded from the study. After excluding children and eliminating children who did not show up for surgery, 208 children were enrolled in the study. The children were randomized by who got which procedure. Once the surgeries were done, results were calculated. The mean closure time of the laser myringotomy was 2.38 weeks, which was calculated from 84 of the 90 percent of patients who appeared to their weekly appointments until closure. In 94 patients, the tube was gone after an average of 3.88 months. For follow-ups after the surgery, “An effusion-free middle ear at the laser side was observed in 46.6% of patients after 1 month and in 35.5%, 37.1%, 38.6%, 41.6% and 39.1% after 2, 3, 4, 5, and 6 months, and for the tube side, this was noticed in 87.4%, 81.9%, 81.5%, 75.5%, 68.5% and 70.7% of patients, respectively.”
The percentages are consistently higher with people who received the laser myringotomy with ear tubes as well. Overall, the study confirmed that laser myringotomy is a safe method to treat chronic ear infections, but proved to be less effective treatment than ventilation tubes. “The laser myringotomy success rate in this trial of approximately 40% (range 46.6 –35.5%) was reached in the first month after the procedure and remained fairly constant over the rest of the follow-up period, whereas the success rate of the ventilation tube showed a significant decrease from 87.4% after 1 month to 70.7% at 6 months (range 87.4 – 68.5%). The effect of the laser myringotomy can therefore be determined 1 month after the procedure.”
Overall, the laser myringotomy is not a bad surgery. It is helpful with reliving ear infections, but the reason tube ventilation is more successful is because the prolonged opening in the eardrum. If the laser myringotomy could be altered to find a way to keep the eardrum open longer, it could prove to be a better and more effective surgery due to the shorter amount of surgery time and lack of general anesthesia, as well as lower costs.