The primary visual pathways in the brain allow athletes to perceive and process visual information. The visual space that healthy athletes can see results from different areas of the brain, or cortical areas, working together to integrate information.
The axons of neurons in the thalamus that travel through the primary visual pathway mediate vision and visual perception. The cortical neurons in the temporal lobe respond to edges in certain orientations or the movement of edges in a particular direction. The primary visual pathway also contains the dorsal and ventral pathways used to process information about faces, shapes, and colors or an object’s relative location and movement.
The Neural Pathway Allowing for Vision
The primary visual pathway is the main neural pathway that allows athletes to see their visual scenes. This pathway’s neural path precedes in the following order: the eye, the thalamus, and the primary visual cortex.
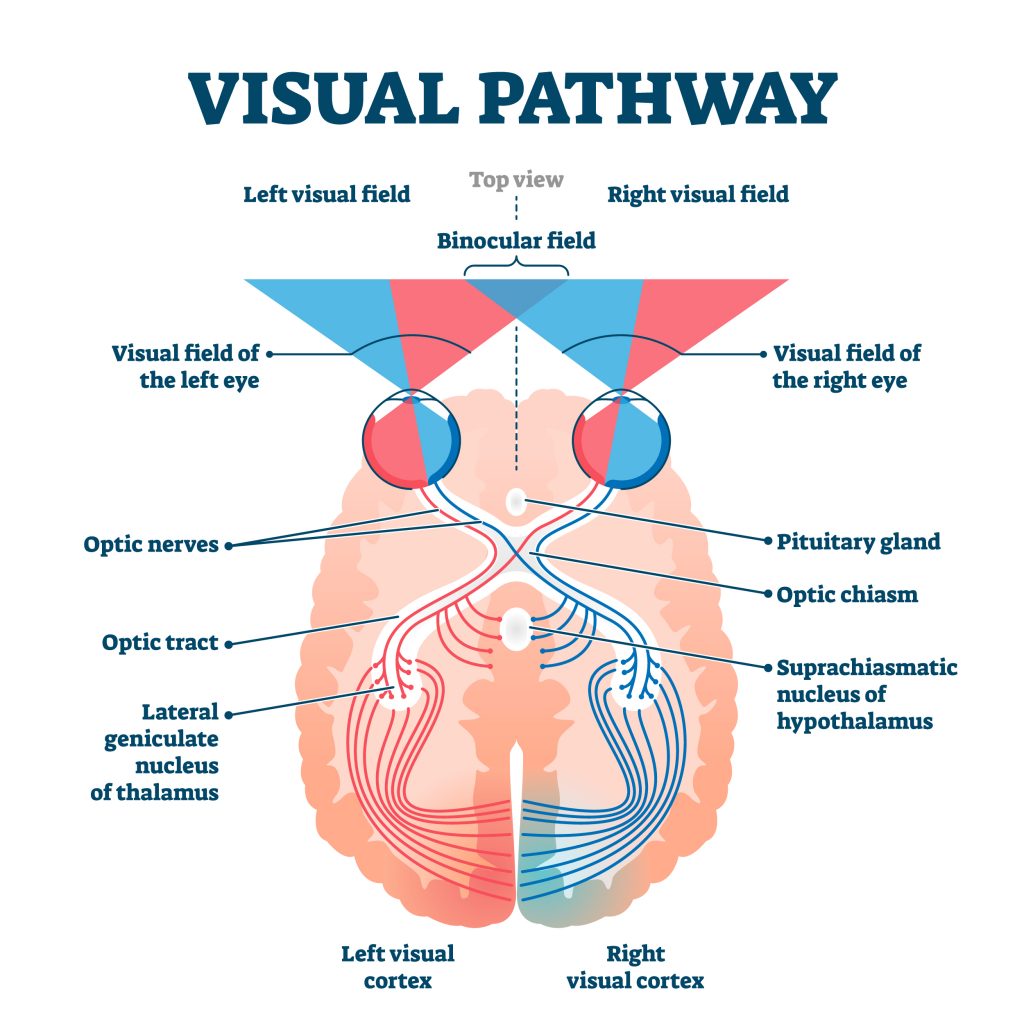
Photo 1: The article Vision, published by Dalhousie University’s Department of Psychology and Neuroscience, displays the primary visual pathway.
Spatiotemporal Tuning of the Neurons in the Visual Cortex– Bars and Edges
Cortical neurons in the temporal lobe respond to the orientation of edges seen in the visual space. Each neuron will have a preferred orientation or movement for edges in a particular direction. When the visual space contains this orientation, the neurons send signals to the brain. Therefore, a specific visual scene is encoded by distinct neurons that respond to certain edges of that visual scene.

Photo 2: The textbook Neuroscience by Dale Purves displays how different orientations of the image of the dog produces the image of the dog seen in the visual scene.
Dorsal and Ventral Divisions in the Primary Visual Pathway
The thalamus is separated into two layers: the magnocellular layer and the parvocellular layer.
| Layer of Thalamus | Cell Type | Convey Information About |
| Magnocellular Layer | M Cell | Motion |
| Parvocellular Layer | P cells | Color |
A study titled “Interactions Between Dorsal and Ventral Streams for Controlling Skilled Grasp” by Vonnevan Polanen found that the connections between these two layers of the thalamus are important for controlling complex object-oriented hand movements in addition to allowing for perception of the visual scene.
Organization of the Extrastriate Visual Areas
The extrastriate visual areas of the brain process other information about a spatial scene. It is organized into the dorsal pathway and ventral pathway.
- Ventral Pathway: The perception of faces, colors, and shapes
- Dorsal Pathway: The location of objects and their movements

Photo 3: The textbook Neuroscience illustrates that the ventral pathway involves the brain’s lower areas. The dorsal pathway involves the brain’s upper areas.