
Thanks for stopping in and learning all about the heart! :]









-
Search It!
-
Recent Entries
-
Links
Thanks for stopping in and learning all about the heart! :]
Posted in All about the heart
This concludes our blog on the cardiovascular system assessment. We have enjoyed blogging on the cardiovascular system. We wish to thank all who have posted comments. We hope that our information was helpful and that our audience is able to use the information we provided in their nursing practice. We also have enjoyed reading the other blogs as we found them informative and can definitely use the techniques we learned. Thank you for visiting our site!

Posted in Uncategorized
TEACHING PATIENTS ABOUT CARDIOVASCULAR EVENTS
Teaching patients about their health conditions and how to improve their daily lives is an important task for every registered nurse. It can be a rewarding experience when our patients follow our instructions and thus experience improvement in their health condition. In order to develop a teaching plan that will be effective, a number of factors should be considered.
If a patient or her family is not educated on what is required, does not understand the importance or has barriers to self-care, they will not participate appropriately in care. The goal of education and counseling is to help patients and caregivers acquire skills and knowledge to better manage their lives. Patient may have a lack of knowledge which results in nonadherence to treatment plans; misperceptions are common. Patient and caregivers should receive individualized education emphasizing self-care. Elements of education should include recognition of worsening symptoms, use of medications, modifying risk factors, diet, and exercise. Physical, cognitive, social, and financial factors should be taken into account when developing an education plan. Assess factors such as barriers to change, readiness to change and internal motivation. Having the patient or caregiver do return demonstrations is an effective way to assess how well the patient understood her care plan.
The following represents some of the more important points to teach patients regarding some commonly experienced conditions involving their cardiovascular health. The list is presented in short points that will be easily understood by your patients. We hope you will find this information informative and be able to use these points in your nursing practice.
(Smeltzer, Bare, Kinkle & Cheever, 2008).
CONGESTIVE HEART FAILURE

STROKE
The American Stroke Association has developed the acronym FAST to assist patients in identifying the symptoms of a stroke.

In addition to FAST the patient should also be aware of the following symptoms which could indicate a stroke is occurring:
HEART ATTACK AND CORONARY ARTERY DISEASE

Some heart attacks are sudden and intense, but most heart attacks start slowly, with mild pain or discomfort. Often people affected aren’t sure what’s wrong and wait too long before getting help. Here are signs that can mean a heart attack is happening:
Calling 9-1-1 is almost always the fastest way to get lifesaving treatment.
(American Heart Association, 2014)
HEART ARRYTHMIAS
Many heart arrhythmias can occur in a patient’s heart. We will provide patient education suggestions for a few of the more common abnormalities.
Atrial Fibrillation

Sinus Bradycardia
EKG SHOWING SINUS BRADYCARDIA

Sinus Tachycardia
EKG SHOWING SINUS TACHYCARDIA

NUTRITION FOR YOUR CARDIOVASCULAR SYSTEM


Posted in All about the heart
Cerebrovascular Accident (CVA)
What is a CVA?
A Cerebrovascular accident is the medical term for a stroke. It is also known as a brain attack. There are two different kinds of stroke; Ischemic Strokes and Hemorrhagic Strokes.
An Ischemic stroke occurs when the blood supply is cut off to a part of the brain. Ischemic strokes are similar to a heart attack where the clot is blocking off blood supply to an adjacent organ. But with a stroke it is happening in the brain.

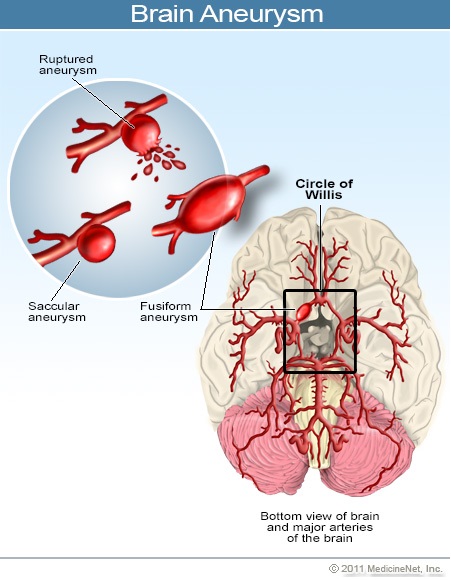
A Hemorrhagic stroke occurs when a blood vessel in a part of the brain becomes weak and bursts open. This causes blood to leak into the brain. Some people have defects in the blood vessels of the brain that make this more likely. These defects may include: Aneurysm and Arteriovenous malformation (AVM).
An aneurysm is a weak point in the blood vessel that may “spring a leak”. AVM is a part of a vessel where part of an artery and vein are malformed and stuck together. Unfortunately, there is high turbulence in this AVM.
RISK FACTORS FOR STROKE
1. High blood pressure
2. Atrial fibrillation
3. Diabetes.
4. Smoking
5. Woman on birth control (higher risk of clotting)
6. Family history of stokes/TIA’s
SIGNS AND SYMPTOMS OF A STROKE

FACIAL DROOP
ARM WEAKNESS
SPEECH DIFFICULTY
TIME TO CALL 911
(If symptoms present)
What is a Transient Ischemic Attack? (TIA)
Many people relate TIA’s to “mini-strokes”. TIA’s are known as mini-strokes because the signs and symptoms that occur are the same, but are temporary, only lasting about a minute. Since the blood flow obstruction to the brain is temporary in a TIA, there usually is no permanent injury to the brain but it is still important to act QUICKLY and get medical help.
THE LONGER YOU WAIT
THE MORE BRAIN MAY BE DAMAGED!
(American Stroke Association, 2014)
(Medicine Net, 2014)
(U.S. National Library of Medicine, 2013)
Posted in Uncategorized
Patent Ductus Arterious
Patent ductus arteriosus (PDA) is a congenital heart defect in which the openings between the pulmonary and aortic valves stay open after birth. The ductus arteriosus serves as a bypass while the child is in utero to bypass the lungs since their blood is oxygenated by the mother. In most cases, the ductus arteriosus closes shortly after birth because the lungs now need to oxygenate the blood. When the ductus stays open the oxygenated and deoxygenated blood mix (Boston Children’s Hospital, 2014).

Symptoms
PDA is the sixth most common birth defect and occurs twice as often in girls than in boys (Boston Children’s Hospital, 2014). A PDA most commonly occurs when the child is premature. The symptoms of PDA depend on the severity of the PDA but are most commonly diagnosed by auscultation of a heart murmur. When a PDA is small, sometimes the child is asymptomatic and is not diagnosed until later in life. If the PDA is more severe, the child may experience fatigue, sweating, rapid or heavy breathing, congested breathing, disinterest in feeding or tiring while feeding, or poor weight gain (Boston Children’s Hospital, 2014).
Outcomes
Some testing that can also be done to diagnose PDA are chest x-rays, echocardiogram, EKG, cardiac catheterization and MRI (Boston Children’s Hospital, 2014). When treatment is needed in newborns, medication is highly effective with few side effects. Indomethacin or ibuprofen is typically the first choice and the earlier the treatment is given, the more likely it is to succeed (ADAM Health Solutions, 2014). If medication is not effective or if the child is too old for medication to be effective, surgery can be performed to ligate the PDA. Another method is coil insertion during cardiac catheterization (Cincinnati Children’s Hospital Medical Center, 2014).
Atrial Septal Defect
Atrial septal defect (ASD) is a condition present at birth. ASD is the third most common congenital defect and is present more often in females than males (Cleveland Clinic, 2014). During fetal development there is an opening in the septum located between the right and left atria; ASD occurs when this opening remains open after birth. Due to this opening, blood flows between both atria which can lead to pulmonary hypertension and heart failure in adults (Mayo Clinic Staff, 2011).

Causes
The exact cause of ASD is unknown but similar to other congenital defects they are thought to be caused by environmental and genetic factors. Evidence shows that diabetes, rubella and lupus are linked to cases of ASD (Cleveland Clinic, 2014).
Symptoms
There are usually no overt symptoms of ASD at birth. A small ASD often resolves on its own during infancy (Mayo Clinic Staff, 2011). Individuals with a large (greater than 2cm) ASD may not begin having symptoms until their 30’s and may be asymptomatic into their 50’s (Cleveland Clinic, 2014). Assessment findings of an individual with ASD include an irregular heart rhythm, heart murmur, shortness of breath, fatigue, edema, frequent lung infections and a bluish skin tone (Mayo Clinic Staff, 2011).
Outcomes
An echocardiogram is used most frequently used to diagnose ASD. Individuals with a detected ASD are treated based on the type, size and the overall effect the defect has on the heart (Cleveland Clinic, 2014). Medications will not assist in closing an ASD but may be used to treat symptoms (Mayo Clinic Staff, 2011). An ASD in those with a high risk of long term complications may be repaired percutaneously with a closure device. Those with more severe forms of an ASD may need open heart surgery for repair (Cleveland Clinic, 2014).
Mitral Stenosis
Mitral stenosis occurs when the mitral valve will not open appropriately. Because the valve does not open properly, blood flow into the left ventricle is impeded during diastole. Overtime, the left atrium enlarges and left atrium pressure is increased (Jarvis, 2012). This occurs from scarring of the mitral valve leaflets and the chordae tendenae. The structures around the valve shorten and thicken which causes a “fish mouth” shape of the mitral valve. Overtime, a pressure difference between the left atrium and ventricle occurs and will eventually cause pressure overload of the left atrium, pulmonary bed, and right ventricle (Lewis, Heitkemper, Dirksen, O’Brien, & Bucher, 2007).

Causes
Mitral stenosis can actually occur in both young children and adults (Davidson, London, & Ladewig, 2008). Although more common in adults it can also be found during infancy or early childhood (Porth, 2007) Oftentimes, the cause is from rheumatic heart disease. Other causes of mitral stenosis include rheumatoid arthritis, and systemic lupus erythematosus (Lewis, et al., 2007). Rheumatic heart disease has greatly declined within the past four decades due to advances in healthcare however still continues to be the main cause of congenital mitral stenosis and results in the most serious lesions. In cases where streptococcal infections go untreated, rheumatic fever may occur. If the heart becomes involved, mitral valve stenosis may develop. During pregnancy, the risk for developing mitral stenosis also increases for the same reasons. Additionally, increased blood volume and the need for increased cardiac output during pregnancy places additional stress on the heart and makes the pregnant client more susceptible to mitral stenosis (Davidson, London, & Ladewig, 2008).
Symptoms
The nurse should be assessing for signs and symptoms such as fatigue, palpitations, exertional dyspnea, and orthopnea (Jarvis, 2012). The main symptom is dyspnea on exertion due to decreased lung compliance. The patient may also experience palpitations, hoarseness, hemoptysis, chest pain, and seizures. Because blood flow is altered and may be obstructed, the patient is at risk for embolization and stroke (Lewis, et al., 2007). When auscultating heart sounds, the nurse should expect to hear a low-pitched murmur. This will often sound like a rumble during diastole. Be sure to auscultate near the apex of the heart (Jarvis, 2012). Using the bell of the stethoscope will help the nurse to better hear the low pitch (Lewis, et al., 2007).
Outcomes
Mitral valve stenosis is a progressive, life-long disorder. The course of the disease starts out slow, however, in later years, signs and symptoms accelerate progressively. As the valve becomes more obstructed, decreased cardiac output occurs and arrhythmias may occur. The normal valve opening is approximately 4 to 5 cm with mild symptoms occurring when narrowing reaches 2cm. Atrial fibrillation occurs in approximately 30-40% of all cases (Porth, 2007).
Posted in Uncategorized
CORONARY ARTERY DISEASE
What is CAD?
Most people develop coronary artery disease (CAD) due to atherosclerosis. Atherosclerosis occurs when plaque made up of fat, cholesterol, calcium, and fibrin form inside of our arteries. High blood pressure, smoking, and cholesterol all can contribute to Atherosclerosis. Our focus is on the arteries that supply the heart muscle.
What happens with plaque buildup?
When plaque settles inside of the artery it cuts off the important blood supply feeding a specific organ, in the case the heart. The blood passing through arteries is very crucial to vital organs; it provides this important muscle with oxygen and nutrients. If this muscle is deprived of oxygen and nutrients it will result in an injury and eventually death. There is a higher risk of clot formation in these arteries if plaque is present.

Why is CAD so important to understand, prevent, and treat?
CAD is the most common form of heart disease, leading cause of death in both men and women in the U.S. CAD can lead to chest pain and a myocardial infarction (heart attack). Medical management can help prevent or delay further plaque formation. An example of surgical treatment would be a coronary artery catheterization with stent placement, allowing the artery to stay open for adequate blood supply to the cardiac muscle.
(National Heart, Lung and Blood Institute, 2013) & (Texas Heart, 2013).
MYOCARDIAL INFARCTION
What is a myocardial infarction?
A myocardial infarction (MI) happens when an artery that supplies oxygenated blood to the heart becomes blocked. The blood is unable to pass through and supply the cardiac muscle properly. The American Heart Association (AHA) estimates that about every 34 seconds an American will have a heart attack.
Causes of a myocardial infarction:
The main cause of a MI is blockage of artery from atherosclerosis with acute clot formation. Spasm of the artery causing occlusion could also occur. Blood flow can also be decreased during times of shock or severe bleeding ultimately leading to inadequate blood supply to the cardiac muscle.

How to prevent a myocardial infarction:
Genetics and family history may cause someone to be at a higher risk for having a MI, but there are also many modifiable risk factors that people can control. These are some of the risk factors that are preventable.
1. Smoking tobacco products. This includes second hand smoke/exposure to smoke.
2. High blood cholesterol. The goal is to have more “good” cholesterol, than bad cholesterol. This can be managed through diet.
3. High blood pressure.This can be reduced with better diet, exercise, stress management, medication.
4. Uncontrolled Diabetes.Checking glucose frequently and properly taking care of your DM through diet and correct medication regimen.
5. Physical inactivity.Exercise is important in overall health and can help prevent the risk of a MI.
What to do during a myocardial infarction:
As nurses, our biggest life saver is education and prevention. It is important to teach our patients the signs and symptoms of a heart attack, the importance of quick treatment, and to call 911 if symptoms do not go away after 5 minutes!
Signs and symptoms include:
Women may experience slightly different sign and symptoms, these include:
If the patient has a nitroglycerin order it’s important to educate them to use them as instructed. If chest pain continues after 5 minutes, remind them to call 911.
If a patient has never experienced this before, educate your patient to chew 1 aspirin or Tylenol and ibuprofen if aspirin is not available until the paramedics arrive.
(Cleveland Clinic, 2013), (National Heart, Lung and Blood Institute, 2013) & (Texas Heart, 2013).
Posted in All about the heart
Congestive heart failure (CHF) is defined 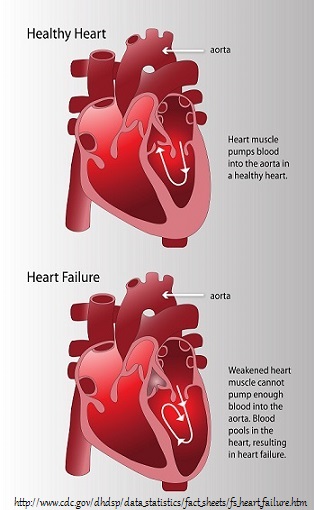 as “an abnormal clinical syndrome involving impaired cardiac pumping and/or filling (Lewis, et al, 2011.)” The primary causes of heart failure include: coronary artery disease, hypertension, congenital heart defects, cardiomyopathy, hyperthyroidism, and valvular disorders. Heart failure can be categorized into left and right sided (Lewis, et al, 2011).
as “an abnormal clinical syndrome involving impaired cardiac pumping and/or filling (Lewis, et al, 2011.)” The primary causes of heart failure include: coronary artery disease, hypertension, congenital heart defects, cardiomyopathy, hyperthyroidism, and valvular disorders. Heart failure can be categorized into left and right sided (Lewis, et al, 2011).
Left Sided Heart Failure
Let’s take a look closer into left sided failure. In left sided heart failure, the left ventricle doesn’t pump effectively. This causes blood to back up into the left atrium and into the pulmonary circulation. As the blood backs up, the pressure rises and causes fluid to escape, which may manifest itself as pulmonary edema. Left sided heart failure is the most common type of failure (Lewis, et al, 2011).
Clinical manifestations that occur during left sided heart failure include: increased heart rate, decreased PaO2 with slightly elevated PaCO2, crackles in the patient’s lungs as well as pleural effusions. Mental status changes and restlessness may also occur. Symptoms that the patient may complain about are weakness, fatigue, anxiety, depression, shortness of breath, shallow, fast respirations, dry, hacking cough, nocturia and paroxysmal noctural dyspnea (Lewis, et al, 2011).
Right Sided Heart Failure
Right-sided heart failure occurs when blood backs up into the right atrium and into the venous circulation. This results in venous congestion, which causes hepatomegaly, splenomegaly, vascular congestion of the gastrointestinal tract as well as peripheral edema. The most common cause of right-sided heart failure is left sided heart failure (Lewis, et al, 2011).
Clinical manifestations that occur during right sided heart failure include: heart murmur, jugular vein distention, edema, weight gain, increased heart rate, ascites, and anasarca. Symptoms that the patient may complain about are fatigue, anxiety, depression, dependent edema of the lower extremities, anorexia and nausea (Lewis, et al, 2011).
DIAGNOSIS
The physician, along with complete history and physical examination, will order some diagnostic tests to aid in the correct diagnosis. A chest x-ray will be ordered, along with a 12 lead EKG, an echocardiogram as well as blood chemistries including a B-type natriuretic peptide (BNP), liver function test and cardiac enzymes (Lewis, et al, 2011).
NURSING ASSESSMENT
Auscultation
When auscultating the client’s heart you may hear tachycardia and murmurs. When listening to lung sounds you may hear crackles, rhonchi and even wheezes. You may also notice they are tachypneic (Lewis, et al, 2011).
Palpation
When palpating the client’s skin you may notice the skin is cool and diaphoretic. You may also notice cyanosis or pallor. When palpating the lower extremities, they may have a pitting edema (Lewis, et al, 2011).
Posted in All about the heart
Assessing For Arrhythmias
Let’s Refresh!
This week we will be looking further at the cardiovascular system and specifically focus on arrhythmias and the heart. Over the past few weeks, we have looked at obtaining a health history related to the patient’s heart, observed the normal heart and circulatory system, and learned ways to assess the extremities and neck vessels. We also learned where to locate the main assessment points of the heart and we learned about nutrition related to the heart. Today we will learn about the electrical conduction throughout the heart and how the heart may be altered if the electrical conduction system is altered.
The Conduction System
Below, is a picture of the conduction system throughout the heart. Impulses within the heart, innervated by nerve tissue, are responsible for depolarization of the heart (causes the heart to contract). In a normal heart, the person’s sinoatrial node (SA node) is responsible for the heart’s electrical impulse. This is the pacemaker of the heart. In many arrhythmias, however, the electrical impulse comes from an area other than the SA node. With normal conduction, the impulse will start with the SA node, located in the atria of the heart. It then travels via internodal pathways to the atrioventricular node (AV node) and then the Bundle of His. From there, the impulse goes to the right and left bundle branches. On the left side, the bundle branch transitions to two fascicles, the anterior and posterior. From here, the heart’s Purkinje Fibers are excited which are located on either side of the ventricle’s walls. All of this happens in approximately 0.12 seconds in the normal heart! Once the impulse has traveled to the Purkinje Fibers a ventricular contraction occurs (Lewis, Heitkemper, Dirksen, O’Brien, & Bucher, 2007).

So What is an Arrhythmia?
In short, it is very important as the nurse, to understand what arrhythmias are. Although the SA node is the normal pacemaker for the heart, cardiac cells in any part of the heart may take on the role of the pacemaker. Arrhythmias are typically categorized according to the site of the pacemaker and therefore include sinus arrhythmias, atrial arrhythmias, junctional arrhythmias and AV blocks and ventricular arrhythmias and bundle-branch blocks. Three commonly seen arrhythmias are sinus bradycardia, sinus tachycardia and atrial fibrillation (Huff, 2012).
The Most Common Arrhythmias
(Below, please find a list of the most common arrhythmias. Without going in depth on each arrhythmia, a rhythm strip is provided for each to better visualize what to expect when heart monitoring is utilized.)
|
Sinus Bradycardia and Sinus Tachycardia Both sinus bradycardia and sinus tachycardia share the same characteristics as that of normal sinus rhythm (rhythm originates in the SA node, P waves are of normal size, shape and direction and precede every QRS complex, PR interval and QRS complexes are normal) with the exception of the heart’s rate. The distinctive feature in sinus bradycardia is a slower rate of 40-60 beats per minute. In sinus tachycardia the rate speeds to a range of 100-160 beats per minute (Huff, 2012).
|
|
Atrial Fibrillation In atrial fibrillation (the most common rhythm seen next to sinus rhythm), electrical impulses originate from an ectopic site in the atria instead of from the SA node. Rapid firing from this ectopic site cause the atria to quiver instead of contracting normally resulting in rapid, irregular and chaotic electrical impulses. Typically the AV node blocks most of the impulses from entering the ventricles resulting in a ventricular rate that is slower than its accompanying atrial rate. Unlike the aforementioned sinus arrhythmias, the rhythm is highly irregular. Because atrial impulses are so rapid, often as fast as 400 beats per minute, P waves are often described as fibrillatory wavy deflections that cannot be counted. The slower ventricular rate (which is less than the atrial rate) is represented by normal QRS complexes but no PR interval is discernable (Huff, 2012). |
|
Ventricular Fibrillation (VF) With this rhythm, the heart’s ventricles serve as the area for electrical conduction. Impulses are disorganized and chaotic, so much that ventricular depolarization and contraction cannot occur. The ventricles instead will quiver, thus creating fibrillatory waves on a ECG strip. VF is the most common cause of cardiac death. Causes of this arrhythmia include myocardial infarction, hypoxia, cardiomyopathy, electrolyte imbalance, and digitalis toxicity. When a person has VF, there is no cardiac output and the nurse will not be able to assess peripheral pulses or blood pressure (Huff, 2012). |
|
Ventricular Tachycardia (VT) This arrhythmia produces impulses at a rate of 140 to 250 beats per minute. VT is most likely caused by reentry into the ventricles, however, may also be caused by heightened automaticity in the ventricles. This occurs during ventricular repolarization. The electrical impulse originates in the ventricle, therefore the SA Node does not act as the pacemaker for the heart, thus no P wave can be visualized. The rhythm is usually regular, however. This rhythm is often seen in patients with heart disease, and in those with a past medical history of coronary artery disease, myocardial infarction, and congestive heart disease (Huff, 2012). |
|
AV Heart Blocks There are several types of heart blocks. A heart block forms when there is a delayed conduction and electrical impulse within the heart or failed conduction through the AV node to the ventricles. With this set of heart blocks, the impulse occurs at either the AV node, the bundle of His, or the bundle branches (Huff, 2012). |
Assessing for the Signs and Symptoms of an Arrhythmia
When assessing the patient for dysrhythmias, the nurse wants to look for several different indicators. Signs of symptoms that the patient may be experiencing if he/she had an arrhythmia includes the following: palpitations, nausea, vomiting, pallor, diaphoresis, weakness, fatigue, numbness and/or tingling of arms, dyspnea, restlessness, cold and clammy skin, dizziness, syncope, confusion, anxiety, decreased level of consciousness, decreased oxygen saturation, either hypotension or hypertension, irregular rate and rhythm of heart, tachycardia, and bradycardia. The patient may also be experiencing pain. Common locations of pain linked with dysrhythmias include the chest, shoulder, back, neck, jaw, and arm (Lewis, et al., 2007).
|
Electrocardiogram (ECG/EKG) An electrocardiogram (ECG/EKG) is a non-invasive test that allows for recording of the electrical activity of the heart. Electrodes placed on the skin allow for detection of the heart’s electrical activity in the form of waves and complexes that can then be displayed on a monitor screen and recorded on ECG graph paper for analysis (Huff, 2012). The ECG allows for the detection of cardiac rhythm, pacemaker activity, conduction abnormalities, and presence of acute injury and myocardial infarct (Lewis, et al., 2007). Below, are two diagrams that show where electrodes are placed on the body when performing an ECG. |
| Cardiac Monitoring
In addition to the performance of a 12 lead ECG, patients can also be monitored on a continual basis during hospitalization with the use of bedside monitoring. Bedside monitoring makes continual observation of the heart’s electrical activity possible and is used to identify abnormalities in rate, rhythm and conduction and to evaluate pacemaker function and responses to various cardiac medications. Continuous monitoring can be achieved by the use of hardwire monitoring or telemetry monitoring. In hardwire monitoring; leads placed on the patient’s chest are then attached via a lead cable system to a bedside monitor, whereas with telemetry monitoring (also referred to as wireless monitoring), leads are attached to a portable monitor transmitter that sends the electrical signals to a central monitor, thereby allowing the patient more freedom of movement (Huff, 2012). In the hospital, on a telemetry setting, cardiac monitors are used regularly. Below is a diagram as to where the electrodes are placed on the patient’s chest.
|
|
Echocardiogram
An echocardiogram, also considered non-invasive testing when used alone, utilizes ultrasound waves to assess the structures of heart valves, chest wall movement, and ejection fraction (Corbett, 2008). The echocardiogram is useful in diagnosing valve abnormalities, congenital cardiac defects, and overall cardiac function. Echocardiogram testing is often combined with other modalities for more detailed information or to obtain more specific information. Examples include stress echocardiogram, pharmacologic echocardiogram and transesophageal echocardiogram (Lewis, et al., 2007). |
|
Holter Monitor
Holter monitors (also referred to as event monitors), are yet another method of assessing a patient’s cardiac status and to help identify arrhythmias. Patients wear a portable recorder that stores information for later printing and analysis. The holter monitor is typically worn for a period of 24-48 hours during which time the patient records a diary of their activity and symptoms. The information from the diary is then correlated to rhythm changes (Lewis, et al., 2007).
|
|
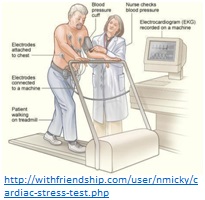
Stress Testing
Exercise stress tests may be used to evaluate the heart’s response to physical stress or increased oxygen demands. In an exercise stress test, the patient exercises on a treadmill or statioanry bicycle while attached to monitoring equipment that measures blood pressure, the person’s ECG, and even oxygen saturation levels. As the patient exercises, he/she is continually assessed by tyrained staff for the developmment of abnormal cardiac symptoms (syncope, vertigo, dyspena, pallor) and ECG changes that may be indicative of myocardial ischemia or arrhythmias (Lewis et al., 2007). |
Questions the Nurse Should Be Asking to Assess for Arrhythmias
· – Sodium Channel blockers such as Dilantin (phenytoin), or -Rhythmol (propafenone)
· –Beta Adrenergic Blockers such as Tenormin (atenolol), -Lopressor (metoprolol), or Betapace (sotolol)
· –Potassium Channel Blockers such as Betapace (sotolol), or -Cordarone (amiodarone)
· –Calcium Channel Blockers such as Cardizem (diltiazem), or Calan (verapamil)
· –Others: Lanoxin (digoxin), or Adenocard (adenosine) (Lewis, et al., 2007)
Other Ways to Assess for Dysrhythmias
Auscultation
Perhaps one of the best ways to assess the conduction system is by directly listening to the heart. Turbulence caused by movement of the valves of the heart creates heart sounds which are heard through the stethoscope. In earlier weeks, we learned about S1 and S2/lub dub sounds. The nurse again wants to use this technique to assess the patient’s current heart rhythm (Lewis, et al., 2007).
Palpation
The nurse should also be using palpation to better assess the patient’s rhythmic status. While simultaneously auscultating the apical area, the nurse should be palpating the radial pulse. The nurse should be feeling for regularity of heart beat. If the apical and radial pulses are not equivalent, one nurse should count the apical pulse while a second nurse counts the radial pulse through palpation. The difference between these two values is known as a PULSE DEFECIT. If the patient is experiencing a pulse deficit, a dysrhythmia is indicated (Lewis, et al., 2007).
WARNING!!
As the nurse, it is important to not rely solely on cardiac monitoring related to cardiac assessment. Computerized monitoring is not fail-proof. When in doubt, check your patient! The heart monitor should not be the only tool the nurse uses to assess the patient’s cardiac status (Lewis, et al.).
Check Out These Videos
1. This video, “Electrocardiogram – What is an ECG – Performing an EKG Video.flv” briefly discusses what an ECG is and why the test is performed. It also discusses a stress test, as well.
2. This video provides an easy to follow visual to better understand how electrical impulses conduct within the heart & the most common dysrhythmias. “The Different Types of Heart Arrhythmia.”
Posted in All about the heart
This week we will be discussing nutrition related to the cardiovascular system. Let’s begin with a quick overview of what nutrition really is. Nutritional status refers to the degree of balance between nutrient intake and nutrient requirements. This balance is influenced by five factors: physiologic, psychosocial, developmental, cultural, and economic (Jarvis, 2012).
Optimal nutritional status is accomplished when adequate nutrients are consumed to support day-to-day body needs and any increased metabolic demands due to growth, pregnancy, or illness. Those with optimal nutritional status are more active, have less physical illnesses, and live longer (Jarvis, 2012).
Undernutrition occurs when nutrients are depleted or when nutrient intake is insufficient to meet day-to-day needs or added metabolic demands. Those at risk for undernutrition include infants, children, pregnant women, recent immigrants, individuals with low incomes, hospitalized people, and aging adults (Jarvis, 2012).
Overnutrition occurs when there is a consumption of nutrients, especially calories, sodium, and fat, in excess of body needs. Overnutrition, which is a major nutritional problem today, can lead to obesity and a risk factor for heart disease, type 2 diabetes, high blood pressure, and stroke (Jarvis, 2012).
Body mass index (BMI) is a numerical value of your weight in relation to your height. This tool is a good indicator to determine if your weight is healthy or unhealthy. Click here to learn more & calculate your BMI (American Heart Association, 2014).
Guidelines for a Healthy Eating Plate:
 (Harvard School of Public Health, 2014)
(Harvard School of Public Health, 2014)
To learn more about creating a healthy meal plate click here(ChooseMyPlate.gov, n.d.).
Risk Factors for Heart Disease that can be Controlled:
Important Questions to Ask:
When performing a nutritional assessment on a cardiac patient, it is important to ask specific questions regarding personal habits as these can be cardiac risk factors. You should ask the patient to describe their usual diet. Take note if this diet is representative of the basic food groups, the amount of calories, cholesterol, and any additives such as salt. You should also ask the patient about their usual weight and if there has been any recent change in weight (Jarvis, 2012).
Additional Important Questions to Ask:
Healthy Tips:
Simple but effective strategies to reduce a patient’s risk for cardiovascular disease include recommending foods such as fish and other lean proteins, fruit, whole grains, and vegetables. Replacing juices and sweeten ed beverages with whole fruit reduces the amount of calories consumed, increases volume and nutrient content, and lowers insulin and triglyceride levels by slowing absorption. Portion control is crucial, as well as limiting foods high in fat, cholesterol, and salt. Thirty to 60 minutes of exercise is recommended on most days of the week to achieve and maintain a healthy weight and to reduce the risk of chronic disease (Olendzki, Speed, & Domino, 2006). To learn more about 25 foods loaded with heart-healthy nutrients that help protect your cardiovascular system click here (WebMD, 2014).
ed beverages with whole fruit reduces the amount of calories consumed, increases volume and nutrient content, and lowers insulin and triglyceride levels by slowing absorption. Portion control is crucial, as well as limiting foods high in fat, cholesterol, and salt. Thirty to 60 minutes of exercise is recommended on most days of the week to achieve and maintain a healthy weight and to reduce the risk of chronic disease (Olendzki, Speed, & Domino, 2006). To learn more about 25 foods loaded with heart-healthy nutrients that help protect your cardiovascular system click here (WebMD, 2014).
To check out more heart-healthy foods, recipes, weight management, stress management, and tips to quit smoking please visit www.heart.org (American Heart Association, 2014).
Posted in All about the heart
Before discussing the assessment of the cardiovascular system let’s first review the anatomy of the heart & major arteries and veins:


(Normal heart, n.d.)
(Circulatory system, n.d.)
PREPARING FOR ASSESSMENT
Before collecting objective data, it is important to first collect subjective data from the patient. When assessing the cardiovascular system be sure to ask the patient if they have any chest pain, shortness of breath, difficulty breathing when laying flat, blue or ashen skin, cough, fatigue, swelling, or frequent voiding at night. Other subjective information should include past medical history, family history and lifestyle. When performing a cardiovascular assessment begin with blood pressure and pulse followed by the extremities, then neck vessels and ending with the anterior chest (Jarvis, 2012).
PERIPHERAL EXTREMITIES
Begin your assessment with inspection and palpation of the arms, followed by the legs. Note the color, temperature and turgor of the skin. In the legs, also assess hair distribution, venous pattern and edema. First check capillary refill of the nail beds; color should return within 1-2 seconds in a healthy individual. Palpate bilateral radial pulses, followed by brachial pulses in the arms. When assessing peripheral pulses, note rate, rhythm, elasticity of vessels and force. Grade the force of the pulses as: 0 (absent), 1+ (weak), 2+ (normal) and 3+ (bounding). In the legs palpate bilateral femoral, popliteal, posterior tibial and dorsalis pedis pulses. Note any edema and grade accordingly (Jarvis, 2012).
 (Pitting edema grading scale, n.d.)
(Pitting edema grading scale, n.d.)
NECK VESSELS
Begin by palpating the carotid artery, do so gently and only on one side of the body at a time. Note the contour which should be smooth and the force which is normally graded 2+. Auscultate carotid arteries in individuals who are middle aged or older or show signs of cardiovascular disease. When auscultating the carotids, listen for a bruit which is an abnormal blowing or swishing sound. In a more advanced cardiovascular assessment jugular venous pulse and pressure may be assessed (Jarvis, 2012).
ANTERIOR CHEST
Begin by inspecting the anterior chest. The apical impulse may be visible at the mitral area (see image below) in children and thin individuals. Palpation of the apical pulse is not always possible particularly in the obese and those with thick chest walls. Continue with palpation across the chest noting the apex, left sternal border and base; pulses should not be present on palpation. Note if a heave, a sustained forceful thrusting (at the sternal border or apex) or thrill, a palpable vibration is present. Auscultate at each of the five assessment points (refer to image). During auscultation note the rate and rhythm, identify S1 (lub) and S2 (dub) and listen for any extra heart sounds or murmurs. Click here to listen to heart sounds. Finish auscultation with placing the patient in the left lateral position and listening with the bell at the apex for any diastolic filling sounds (Jarvis, 2012).
forceful thrusting (at the sternal border or apex) or thrill, a palpable vibration is present. Auscultate at each of the five assessment points (refer to image). During auscultation note the rate and rhythm, identify S1 (lub) and S2 (dub) and listen for any extra heart sounds or murmurs. Click here to listen to heart sounds. Finish auscultation with placing the patient in the left lateral position and listening with the bell at the apex for any diastolic filling sounds (Jarvis, 2012).
(Locating the assessment points, n.d.)
PUTTING IT ALL TOGETHER
(Hippocratv, 2013)
Posted in All about the heart
During care for a patient, it is important to have a complete health history. This allows for the patient to receive proper care while co nsidering their previous or underlying conditions. This is also important to determine if they have had previous care for similar conditions and what worked well for them in the past.
nsidering their previous or underlying conditions. This is also important to determine if they have had previous care for similar conditions and what worked well for them in the past.
It is important to start the health history by obtaining their name, date of birth, gender, contact information, race, ethnic origin, and occupation. Much of this information has been gathered by the time the patient sees the nurse but still deserves mentioning for those cases that this information is not yet collected. Nurses also need to consider this information and determine if the patient will need assistance with and communication barriers, whether it be a language barrier or if the patient needs assistance with hearing or seeing.
While collecting the health history, document who is providing you with the information, if they are reliable and if any special circumstances occurred, such as utilizing an interpreter or devices for the  hearing impaired. This allows for others to read the information and understand what was occurring at the time of the interview. Also include why the patient sought treatment and use the patient’s words in quotation whenever possible.
hearing impaired. This allows for others to read the information and understand what was occurring at the time of the interview. Also include why the patient sought treatment and use the patient’s words in quotation whenever possible.
When discussing the patient’s present illness, it is important to ask them when it started and what has occurred since, and why they decided to seek treatment that day if it has been an ongoing problem. Also ask them how they view their health; do they find themselves to be overall healthy or sickly?
After discussing their current illness, it is also important to discuss their previous illnesses. Health history needs to include childhood illness, accidents or injuries, chronic conditions, previous hospitalizations, surgical history, obstetrical history, immunizations, allergies, and last related exam, depending upon illness or complaint. The more complete the health history, the better care we can provide.
Once we have established the patient’s personal history, family history also needs to be considered. By understanding the family history of certain diseases, we can assess the patient’s risk for these conditions. We can also use this to educate our patients to prevent them from developing certain diseases or reduce the impact of these diseases. In addition, a patient’s culture needs to be con sidered for their religious and spiritual practices and beliefs and restrictions. Are there any restricts on treatments, testing or foods?
sidered for their religious and spiritual practices and beliefs and restrictions. Are there any restricts on treatments, testing or foods?
Discussion of the home life is also important during the collection of the health history. Are they able to care for themselves or is someone there to help them? Do they feel safe at home or are they being abused? Do they smoke and does it occur in the home? Who is their support system? Also consider their occupation when considering any occupational hazards or exposures.
There are times in which a patient is unable to provide their health history. If this occurs we need to utilize medical records on the patient or discuss the history with the family, as long as they are reliable.
Below are two examples of health history forms that can be utilized to collect information. Check them out!
Health History- Includes Cultural Variances
Health History- Extensive Past Medical & Family History
By acquiring a comprehensive health history, we ensure that everything is “on the table”. When discussing health history with patients, we need to ensure them that they can trust us with this information and it will be used to help treat them. By creating a trusting relationship with our patients, the more likely they are to trust us with this information.
(Jarvis, 2012)
Posted in All about the heart