As we normalize talking about mental health, many are raising awareness about more common disorders like anxiety and depression. However, there is a lack of awareness surrounding less common mental health disorders, so I have decided to start a series in which we cover less well-known disorders. Today, we will talk about an eating disorder called avoidant-restrictive food intake disorder, or ARFID. ARFID was first introduced in the DSM-5 in 2013, and many people do not fully understand the disorder, even as awareness of ARFID is increasing.
When thinking about eating disorders, most people picture someone changing their eating habits in order to lose weight or alter their body in some way. While many eating disorders, such as anorexia nervosa and bulimia nervosa, fit this description, not all eating disorders do. For example, those with ARFID do not restrict their food intake with the goal of losing weight. Rather, eating can be physically and emotionally difficult for these individuals, causing them to consume less food or limit their diet to certain types of foods.
What is ARFID?
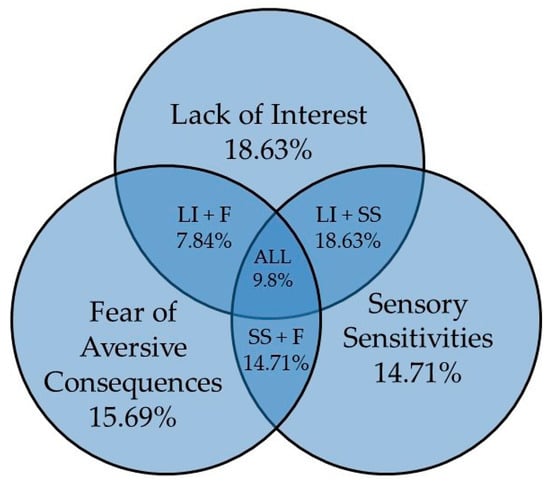
Fig. 1. Nutrients.
Those diagnosed with ARFID have trouble meeting nutritional and/or energy needs for any of the following reasons:
- Lack of interest in eating or food: those with ARFID may say that they have no appetite, don’t enjoy eating, or are full after eating a small amount.
- Avoidance based on sensory characteristics of food: those with ARFID may avoid or eat foods only of certain texture, taste, smell, temperature, or appearance.
- Concern about aversive consequences: those with ARFID may have a fear of choking or vomiting.
To be considered ARFID, the restrictive eating pattern must affect the individual in at least one of the following ways:
- Significant weight loss
- Need for enteral feeding (tube feeding)
- Severe nutritional deficiency
- Negative impact on psychological/social functioning

Comorbid ASD and ADHD
ARFID is linked to neurodevelopmental disorders, particularly autism spectrum disorder (ASD) and attention deficit hyperactivity disorder (ADHD). One study found that among patients with ARFID (n=263), comorbid ASD was present in 58.3% of patients relative to 41.7% in the non-ARFID group (Fig. 2). Sensory sensitivities common to those with autism and ADHD contribute to the acceptance or refusal of food because of texture, presentation, temperature, color, or smell.
ARFID Statistics
The prevalence of ARFID in the general population is not known. However, it is known that the rates of ARFID are between 5% and 14% in pediatric inpatient eating disorder programs and up to 22.5% in a pediatric eating disorder day treatment program. ARFID also affects more males than females, and it is more common in children and young adolescents and less common in late adolescence and adulthood.
Treatment
The most appropriate level of care for treatment depends on the patient’s overall health. Eating disorder treatment may include inpatient-level care, residential-level of care, partial/intensive outpatient programs, or outpatient therapy. The treatment process for ARFID typically involves providing education about the diagnosis, treatment, and importance of nutrition as well as monitoring food intake and increasing volume and/or a variety of fear foods.