
As of mid-2022, COVID-19 had infected more than 500 million people worldwide. The latest estimates show that global “excess deaths” directly and indirectly attributable to COVID-19 could have been as high as 15 million by the end of 2021. The pandemic has severely disrupted essential health services, triggered an increase in the prevalence of anxiety and depression, lowered global life expectancy, derailed progress towards ending HIV, tuberculosis (TB) and malaria, and halted two decades of work towards making health coverage universal.
 Loading...
Loading...
Loading...
Loading...
The burden of disease on life by country:
“The sum of mortality and morbidity is referred to as the ‘burden of disease’ and can be measured by a metric called ‘Disability Adjusted Life Years‘ (DALYs). DALYs are measuring lost health and are a standardized metric that allow for direct comparisons of disease burdens of different diseases across countries, between different populations, and over time. Conceptually, one DALY is the equivalent of losing one year in good health because of either premature death or disease or disability. One DALY represents one lost year of healthy life.”
Types of diseases:
| Communicable, maternal, neonatal and nutritional diseases | Non-communicable diseases (NCDs) | Injuries |
|---|---|---|
| Diarrhea, lower respiratory & other common infectious diseases | Cardiovascular diseases (inc. stroke, heart disease and heart failure) | Road injuries |
| Neonatal disorders | Cancers | Other transport injuries |
| Maternal disorders | Respiratory disease | Falls |
| Malaria & neglected tropical diseases | Diabetes, blood and endocrine diseases | Drowning |
| Nutritional deficiencies | Mental and substance use disorders | Fire, heat and hot substances |
| HIV/AIDS | Liver diseases | Poisonings |
| Tuberculosis | Digestive diseases | Self-harm |
| Other communicable diseases | Musculoskeletal disorders | Interpersonal violence |
| Neurological disorders (including dementia) | Conflict & terrorism | |
| Other NCDs | Natural disasters |
Inequality and reform
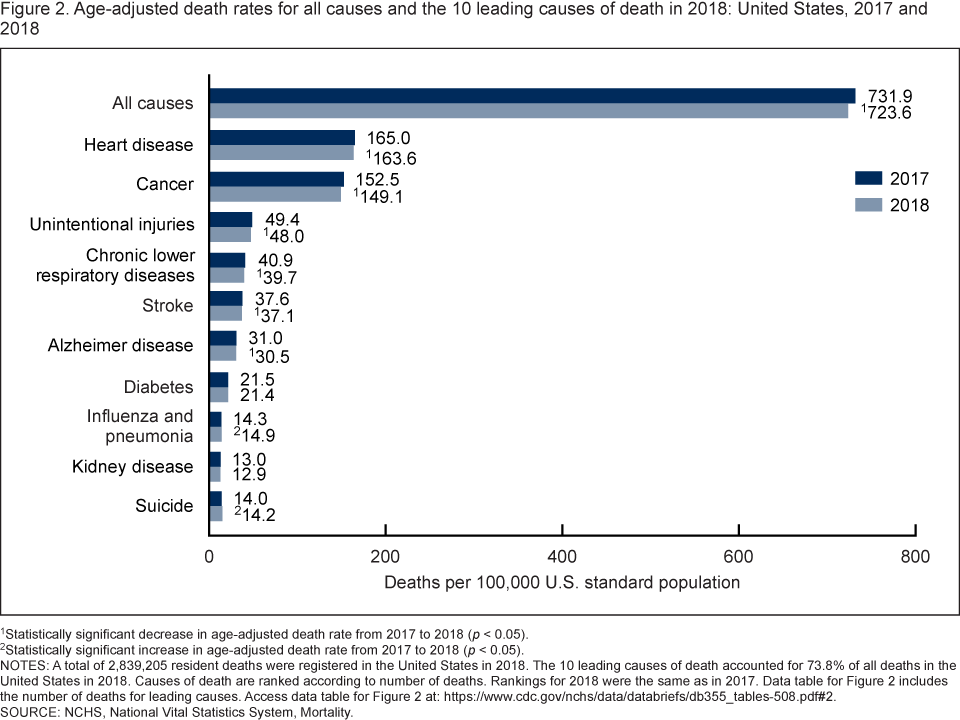
Progress in treating human disease in their different types will come from addressing the systematic externalities they stem from. There is sufficient data to show that Communicable, maternal, neonatal and nutritional diseases are prominent in lower-income countries, for example the Congo’s top 10 causes of death include 9 communicable diseases, in contrast the US does not have a single communicable disease in the top 10. The intrinsic nature to survive communicable disease comes from wealth, established health care systems, environmental regulations, and better standard of living. The closing of these gaps will require not only an international effort, but reforms that are suitable for that country’s needs whether it be the high-costs of healthcare, inability to get insurance, lack of hospitals and infrastructure, or poor hygiene.
{kind=link}
Our world has made admirable progress on saving lives taken from communicable disease (1.1 billion in 1990 to 670,000 in 2016), but even when development comes the issues of treating communicable diseases must be dealt with properly (with pit falls such as vulnerability in health care coverage, high costs of treatment medicine, or differences in rural and urban healthcare.)