When looking at the current state of sex education in America, some questions immediately come to mind. How did this come about? Who decides what kind of sexual education is taught in schools and what material needs to be covered or stressed? What persons and agencies have an influence on public sex ed and can potentially make improvements to it?
The answer is, as always, complicated. There is no one single person or department that decides the fate of sexuality education in America. Rather, there is a variety of influences that act on several levels: federal, state, and local. Each one has a potential to make a difference, but some agencies are better equipped to have a significant effect on sex ed in schools. Below is a brief overview of the main actors:
Federal: The U.S. federal government does not have a direct role in sexual education. As prescribed in the Constitution, education in general is largely a state and local responsibility. Thus, the federal government has little control over what is taught in public schools. However, federal agencies can still influence education through their allocation of funding.
Sex education specifically is funded not through the Department of Education, but through the Department of Health and Human Services, which distributes funds to school systems and community-based agencies. From 1996-2010, over $1.5 billion in federal funding was spent on abstinence-only programs. Since then, abstinence-only programs have been found ineffective, but while their federal funding decreased, $50 million is still spent every year to fund abstinence-only sex education.
Beginning in 2010, two sources of federal funding for comprehensive sex education became available: The Personal Responsibility Education Program (PREP) and The President’s Teen Pregnancy Prevention Initiative (TPPI). Both of these programs grant funding to schools and public agencies that implement medically-accurate, evidence-based programs that cover both abstinence and contraception. This is certainly a step in the right direction. However, while funding can encourage more schools to teach comprehensive sex ed, it cannot solve the issue of inconsistency: it is possible that within one state one or two schools will teach comprehensive sex ed to receive these federal funds, while the rest cover abstinence-only sex education or none at all.
State: State government has the most power in determining sex education in its state. States can mandate that sexuality education be taught, require schools to teach about STDs or HIV/AIDS, set state-wide guidelines for topics, choose curricula, and approve textbooks. These mandates and guidelines can be either governed by law, as passed by state legislature and signed by the governor, or established by the State Department of Education. State departments of education are also generally responsible for disbursing state and federal funds to local school districts, so they have the power to monitor how the programs are being implemented before distributing the funds.
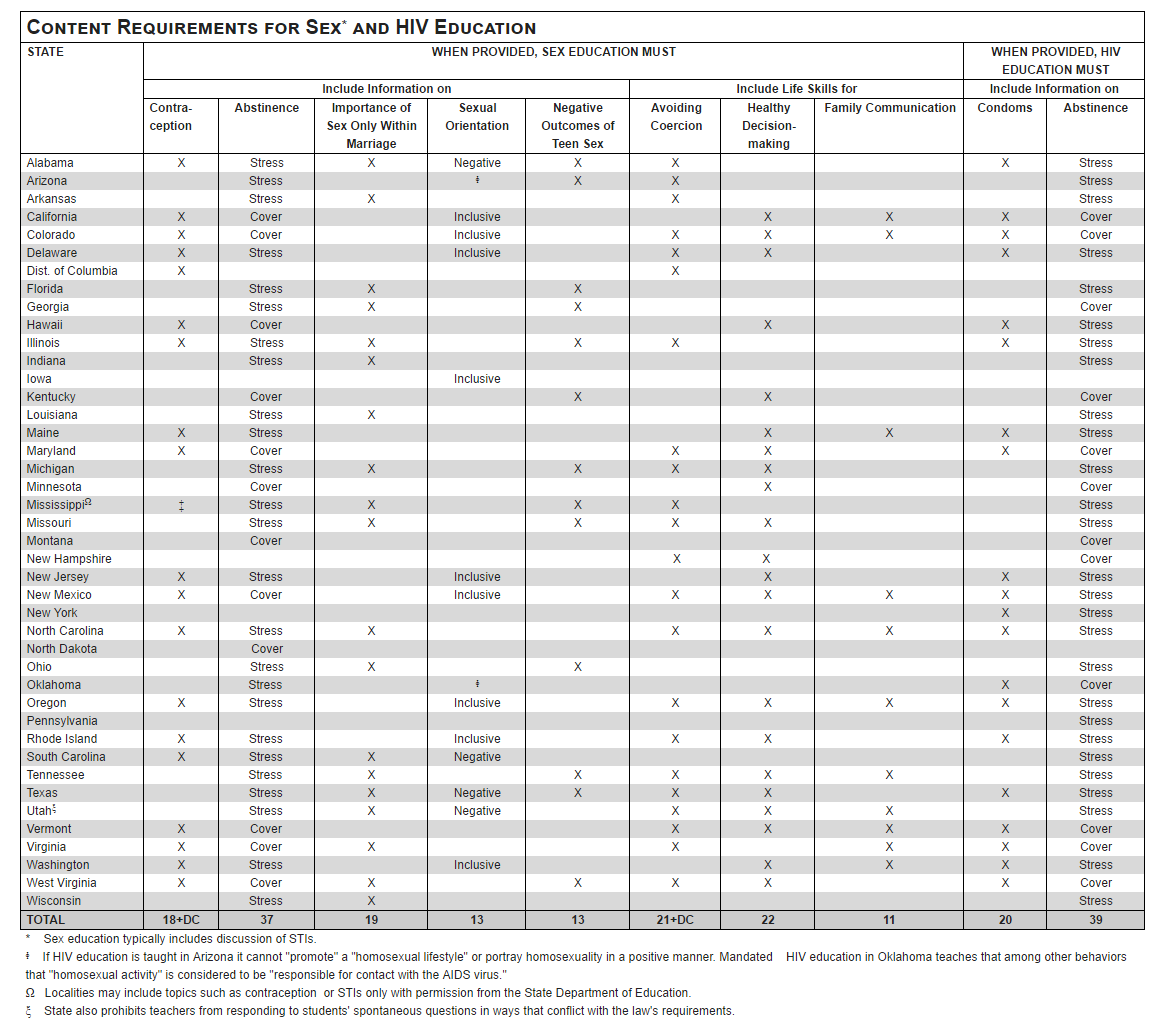
Because the most important decisions about sexual education are made at this level, sex ed policy varies greatly by state. Each state has the right to create its own mandates on whether or not sex education is required, what kind of content is to covered, and how the material should be presented. As discussed in the previous post, this creates a lot of inconsistency in terms of what students can expect to learn depending on where they live.
Local: On the local level, decisions are made by school boards, administrators, and teachers. Some districts also create special advisory committees that determine what content is covered in health and sexuality courses in public schools. Teachers, clergy, public health officials, parents, and even students can make their voices heard in these advisory boards.
Local school boards have the authority to determine the school district budget and priorities, dictate the sequence and scope of the curriculum, and approve textbooks for school courses. All the standards and requirements set by school boards must comply with state law. Thus, it is also a local responsibility to ensure that schools teach sex ed programs that satisfy state policy and any other requirements if they receive additional funding. Overall, local agencies such as school boards can expand on sexuality education that is required by the state, but they cannot institute any changes in violation with existing policy.
In conclusion, there are many agents that affect public sex education, with the most powerful being the state. But that also means that there are many different ways to bring about change. Whether it’s the federal government that directs all sex ed funding towards comprehensive education, state law that mandates content on contraceptives, or a student who advocates for accurate and useful sex ed courses on an advisory committee, there are many opportunities to make a difference. And I’m hopeful that one day all students will have access to the education they need to lead healthy and happy (sex) lives.
“Sexuality Education Q & A.” SIECUS. Sexuality Information and Education Council of the United States, Web. 08 Apr. 2017.
Bridges, Emily, and Debra Hauser. “Youth Health and Rights in Sex Education.” Future of Sex Education. Advocates for Youth, May 2014. Web. 08 Apr. 2017.