
When we were told to create a blog based on a subject which may occur in our lives which we could apply some of the theories we have been learning about I immediately thought of an occurrence which happens almost everyday at my work. I work as a certified drug and alcohol counselor. When clients come to me they normally have a few commonalities. First they have a diagnosis of a substance abuse disorder that has had a very serious negative impact on their lives. Second following the diagnosis of substance abuse they normally have a diagnosis of depression. I see these two diagnosis’s working against one another. They use substances to help cope with their depression but the substance use causing negative consequences makes for more serious depression. In drug and alcohol counseling we call this being in a state of terminal hopelessness where a person can not imagine life without the use of drugs or without being severely depressed and feels trapped. I would like to identify how the hopelessness theory of depression and the self-efficacy theory could help bring about hopefulness for these clients.
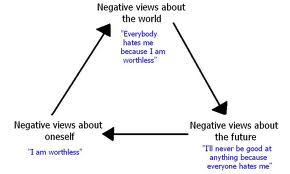
The hopelessness theory of depression has a causal model associated with it which ends with hopelessness. Hopelessness is defined as “the expectation that highly desirable outcomes will not occur and that one is powerless to change the situation” (Schneider). In the causal model my clients generally would experience something like this. First they would start using drugs and alcohol either to cope with an earlier negative life event or as a social coping mechanism. As time goes on negative outcomes of the drug use such as being arrested begin to build a pattern starting to establish a negative view of oneself. As this pattern continues the client begins to believe that these events are of high importance and are creating who they are. As this goes on there drug use begins to effect others and they begin to lose social support. The client begins to blame others for the negative circumstances in their lives because they are trying to fight off the negative views of themselves. This ends up as a negative view of the world and people who used to be their primary support. As this pattern continues the client begins to believe that the future will hold more of the same negative outcomes. These negative views of oneself, the world, and the future brings about the hopelessness theory of depression. Also associated with hopelessness depression is a low self worth, low self esteem, lack of motivation, and a overdependence on people or in this case drugs and alcohol. The client believes they are stuck in a cycle which is impossible to get out of. So the question is how can a hopefulness therapy and self-efficacy help improve the functioning of these individuals.
Hopefulness therapy is designed to help people set goals and help people find ways around barriers to achieve them (Cheavens). Setting small goals also help raise a persons motivation which is much needed in a person with hopeless depression. An example for my clients would be beginning to plan their day setting a few small goals. Returning in a week show the clients how much those small goals helped them achieve in just a week. Another example would be if a client did not have transportation to find employment help them look into public transportation schedules and resources for free bus tokens to remove that barrier so they do not continue to feel stuck. It also helps people identify their strengths and use them for a new direction in their lives. There has been studies done on this type of therapy done at Ohio State University which have shown improvements in functioning for people with this therapy.
In conjunction with hope therapy with my clients, the use of the self-efficacy theory which was developed by Bandura seems to be a good application. Self-efficacy helps people believe in their capabilities to overcome difficult tasks rather than avoid them (Bandura Pg. 231). Which overcoming a drug and alcohol addiction and depression can be extremely difficult. Research has shown multiple ways to improve self-efficacy and I will focus on one. Seeing others that are similar to the client that have succeeded in sustained success in overcoming addiction and depression helps improve self-efficacy. With my clients the group setting motivates them to feel they are not alone in trying to overcome there issues but I have found that suggesting a client to attend 12 Step meetings lets them experience people who have sustained success which helps them find hope and therefor raise self-efficacy. It also helps that 12 Step programs have been showed to be successful for over 80 years now. I find that knowing that it has a long history of being successful means that clients will get to experience people who have had long term success.
The application of these two theories as modes of therapy will bring about lessoned symptoms of depression, lower drug and alcohol use, and therefore overall functioning. Because both of these approaches have research which shows success that these are good theories to apply to a current life situation that I have working with my clients. It helps also that these practices have already been being used. It helps understand where research has been done and has seen success to use these approaches more often and gain understanding of how they can be applied in a more successful manner.
Bandura, A. (1991a). Self-efficacy mechanism in physiological activation and health-promoting behavior. In J. Madden, IV (Ed.), Neurobiology of learning, emotion and affect (pp. 229- 270). New York: Raven.
Cheavens, J. (2014, August 16). YOU’VE GOT TO HAVE HOPE: STUDIES SHOW “HOPE THERAPY” FIGHTS DEPRESSION. Retrieved September 14, 2014, from http://researchnews.osu.edu/archive/apahope.htm
Schneider, F. (2012). Applying Social Psychology to Clinical and Counseling Psychology. In Applied social psychology: Understanding and addressing social and practical problems (2nd ed.). Thousand Oaks, Calif.: SAGE Publications.
Hello! I found your post interesting, and I could not help but wonder if you have ever worked with veterans that are suffering from PTSD? I know most veterans suffering from PTSD engage in dangerous behavior and often times become addicted to drugs and alcohol. I was curious that if you did/do work with them, if you see a difference in how the 12 step process affects them when compared to those that do not necessarily have the underlying PTSD to try and cope with too?
Going through the chapters and the commentary this week, it was a continuous question in the back of my mind on whether or not the material applies to those with PTSD, and how it can apply because I almost feel like PTSD is a separate beast of its own in comparison to the everyday common problems the book ties into the different theories.